Anatomy of the Caudal space
Caudal analgesia is produced by injection of local anaesthetic into the caudal canal. This produces block of the sacral and lumbar nerve roots. It is useful as a supplement to general anaesthesia and for provision of postoperative analgesia. This technique is popular in paediatric patients. Catheter insertion may be performed for continuous caudal block.
Anatomy
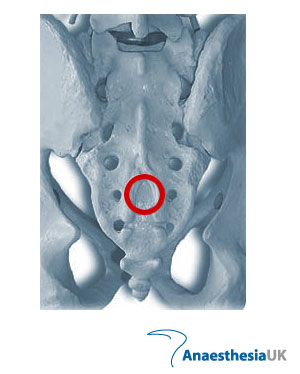
The sacrum is a triangular bone that articulates with the fifth lumbar vertebra, the coccyx and the ilia. The dorsal roof consists of the fused laminae of the five sacral vertebrae and is convex dorsally. In the midline is a median crest which represents the sacral spinous processes. Lateral to this is the intermediate sacral crest with a row of four tubercles which represent the articular processes. The S5 processes are remnants and form the cornua, which provide the main landmarks for indentifying the sacral hiatus. The hiatus is covered by the sacro-coccygeal membrane. The canal contains areolar connective tissue, fat, sacral nerves, lymphatics, the filum terminale and a rich venous plexus.
Technique
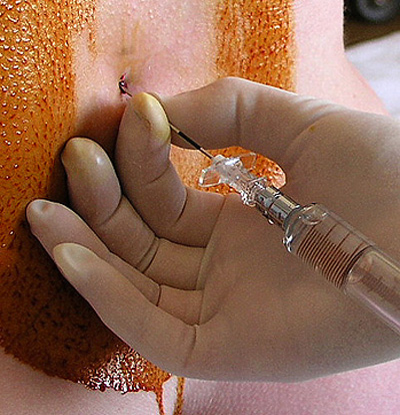
The patient is usually in the left lateral position with the knees drawn up to the chest. The sacral hiatus lies at the third point of an equilateral triangle formed with the two posterior superior iliac spines (look for the dimples in the skin). The cornua are palpable on either side of the hiatus. Adopt an aseptic technique. A needle (or 22/20 g cannula) is introduced in a slightly cranial direction through the hiatus. A click is felt as the needle pierces the sacrococcygeal membrane. The needle/cannula is then directed cranially. The dura ends at S2, but may extend further. Aspirate to confirm the absence of blood/cerebrospinal fluid and inject local anaesthetic while feeling for inadvertent subcutaneous injection with the other hand. There should be very little resistance to injection. In children, the block should be performed after general anaesthesia has been induced and before surgery has commenced.
Choice of local anaesthetic
Paediatric population
0.5 ml/kg, 0.25% bupivacaine (sacro-lumbar block)
1 ml/kg, 0.25% bupivacaine (upper abdominal block)
1.2 ml/kg,0.25% bupivacaine (mid-thoracic block)
(Doses described by Armitage).
In this age group, epidural analgesia is accompanied by very little change in blood pressure or cardiac output. Continuous caudal catheters have been used intraoperatively for more prolonged surgery. The maximum safe dose range for epidural bupivacaine is 0.15-0.2 mg/kg/h in neonates and 0.2-0.3 mg/kg/h in infants. The addition of clonidine (1-2 mcg/kg) to bupivacaine extends its duration of action significantly. Preservative-free Ketamine (0.5 mg/kg) also prolongs the duration of analgesia.
Adult population
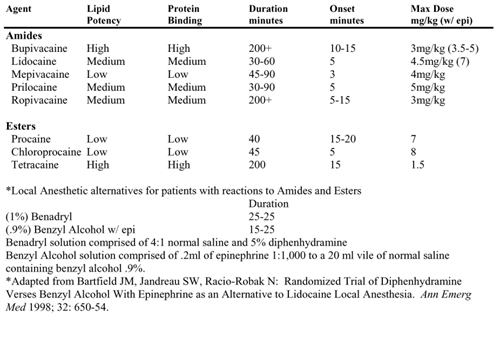
20-30 ml 0.25-0.5% bupivacaine. Average volume of the sacral canal is 30-35 ml.
Epidural fat in children has a loose and wide-meshed texture, whereas in adults it becomes more densely packed and fibrous. Hence, local anaesthetic spread is greater in children.
References
i] Caudal bupivacaine and s(+)-ketamine for postoperative analgesia in children.
Weber F, Wulf H.
Paediatr Anaesth 2003; 13(3): 244-8.
ii] The 'swoosh' test--an evaluation of a modified 'whoosh' test in children.
Orme RM, Berg SJ.
Br J Anaesth 2003; 90(1): 62-5.
 Local anesthesia is a type of pain prevention used during minor procedures to numb a small site where pain is likely to occur without changing the patient's awareness.
Local anesthesia is a type of pain prevention used during minor procedures to numb a small site where pain is likely to occur without changing the patient's awareness. In accordance with the usual practice after a neuromuscular block, we recommend that you monitor the patient in the immediate post-anesthesique period to detect the
In accordance with the usual practice after a neuromuscular block, we recommend that you monitor the patient in the immediate post-anesthesique period to detect the

 Whether you know if the animal you are about to work on is contagious or not, the antibacterial filter protects your anesthesia machine and future patients from possible contamination.
Whether you know if the animal you are about to work on is contagious or not, the antibacterial filter protects your anesthesia machine and future patients from possible contamination.  GlideScope® Video Laryngoscopes offer an improved approach to airway management. GlideScope® provides a consistently clear view of the airway, enabling quick intubation, and offers significant benefits to Anesthesiology, Surgery, and Emergency Medicine markets. Its robust design, long-lasting rechargeable battery, large viewing monitor and several blade sizes are all contributing factors making the GlideScope® the market leader in video laryngoscopy
GlideScope® Video Laryngoscopes offer an improved approach to airway management. GlideScope® provides a consistently clear view of the airway, enabling quick intubation, and offers significant benefits to Anesthesiology, Surgery, and Emergency Medicine markets. Its robust design, long-lasting rechargeable battery, large viewing monitor and several blade sizes are all contributing factors making the GlideScope® the market leader in video laryngoscopy Hearing soothing music while under anesthesia eases patients’ recovery after surgery — results of a Swedish study suggest. According to findings published in a recent issue of a journal, ACTA, Anaesthesiologica Scandinavica, women undergoing hysterectomies, under general anesthesia, who listened to relaxing music and sounds of ocean waves, experienced less pain and were less fatigued, when discharged from the hospital. They were able to sit up sooner after their operation than patients, who did not listen to such music.
Hearing soothing music while under anesthesia eases patients’ recovery after surgery — results of a Swedish study suggest. According to findings published in a recent issue of a journal, ACTA, Anaesthesiologica Scandinavica, women undergoing hysterectomies, under general anesthesia, who listened to relaxing music and sounds of ocean waves, experienced less pain and were less fatigued, when discharged from the hospital. They were able to sit up sooner after their operation than patients, who did not listen to such music.  the hallmark pathologic findings. There are also changes in synapses and the activity of multiple major neurotransmitters, especially involving acetylcholine and central nervous system nicotinic receptors. Two types of Alzheimer's disease have been described: early onset and late onset. Early-onset Alzheimer's disease usually presents before age 60 and is thought to be due to missense mutations on up to three genes leading to an autosomal dominant mode of transmission. Late-onset Alzheimer's disease usually develops after age 60, and genetic transmission appears to play a relatively minor role in the risk of developing this disorder. With both forms of the disease, patients typically develop progressive cognitive impairment that can consist of problems with memory as well as apraxia, aphasia, and agnosia. Definitive diagnosis is usually made on postmortem examination, usually making premortem diagnosis of Alzheimer's disease one of exclusion. There is currently no cure for Alzheimer's disease, and treatment usually focuses on control of symptoms. Pharmacologic options include cholinesterase inhibitors, such as tacrine, donepezil, rivastigmine, and galantamine.
the hallmark pathologic findings. There are also changes in synapses and the activity of multiple major neurotransmitters, especially involving acetylcholine and central nervous system nicotinic receptors. Two types of Alzheimer's disease have been described: early onset and late onset. Early-onset Alzheimer's disease usually presents before age 60 and is thought to be due to missense mutations on up to three genes leading to an autosomal dominant mode of transmission. Late-onset Alzheimer's disease usually develops after age 60, and genetic transmission appears to play a relatively minor role in the risk of developing this disorder. With both forms of the disease, patients typically develop progressive cognitive impairment that can consist of problems with memory as well as apraxia, aphasia, and agnosia. Definitive diagnosis is usually made on postmortem examination, usually making premortem diagnosis of Alzheimer's disease one of exclusion. There is currently no cure for Alzheimer's disease, and treatment usually focuses on control of symptoms. Pharmacologic options include cholinesterase inhibitors, such as tacrine, donepezil, rivastigmine, and galantamine. Anesthesia
Anesthesia  ,
,
 about your pain level.
about your pain level.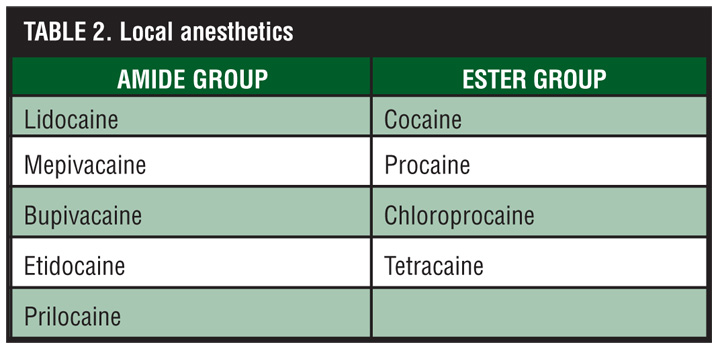



 Spinal Anesthesia Side Effects
Spinal Anesthesia Side Effects




 وبلاگ تخصصی بیهوشی
وبلاگ تخصصی بیهوشی{kind=link}